26 May MEMBERSReversibly screw-retained and metal-free single tooth restoration

Reversibly screwed and
metal-free single-tooth restoration
Case Report
In December 2016, a 43-year-old female patient in good general condition and with the desire for metal-free restoration of the existing single tooth gap regio 36 in our practice. Tooth 36 was already removed by her family dentist in September 2016.

Selection of the implant
In implantology with titanium implants, two-part systems with screwed abutments are considered the gold standard today. They cover almost all indications, allow unloaded healing phases and one-stage augmentation procedures. They are reversible and flexible.
The trend and the development of ceramic implants is analogous to two-part screw-retained solutions. In the present case too, a metal-free, screw-retained, two-part implant system made of zirconium oxide was used (Zeramex P6).

Fig. 1: Implant planning in DVT and SMOP software.

Fig. 2: Insertion of the implant by hand.
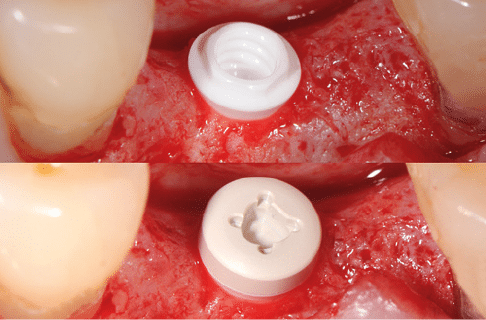
Fig. 3: Implant in situ / healing cap in situ.
Diagnostics
The implantological diagnostics and the implant selection were carried out using DVT. Template-navigated implant placement was dispensed with in this case for reasons of cost and to keep the situation manageable. However, we checked the implant position with the Guided Surgery Software (SMOP, Swiss Meda). The alveoli of tooth 36 were still clearly visible three months after tooth removal. However, sufficient bone conditions and a sufficiently wide distance to the mandibular nerve were shown so that an implant with Ø 4.1 mm and a length of 10 mm could be selected (Fig. 1). It should be noted that this implant type was designed as a classic tissue level implant, i.e. the implant shoulder should be placed epigingivally in the posterior region up to a maximum of one millimeter subgingivally.

Fig. 4: Transmucosal wound closure.

Fig. 5: Control recording four months postoperatively/control restorative treatment (2017)/control recording 2 years after restorative treatment (2019).

Fig. 6: Unattractive soft tissue conditions after exposure.
Surgical phase
At the end of January 2017, the implants were inserted under local anesthesia. After a crestal incision without vertical incisions a well regenerated cortical bone was visible after unfolding. The implant site was prepared in stages according to the drilling protocol. The most important step in preparation is the use of the tap. Since the implants are not self-tapping and the ceramic material does not conduct temperature from the depth, the thread must be cut through to the full length of the implant. Accordingly, the implant should be inserted by hand at the beginning with as little torque as possible (Fig. 2). Only in the last two to three rotations does the implant begin to maintain its primary stability and can then be tightened with a torque of up to 25 Ncm. Since the gingiva thickness was less than two millimeters and penetration of the implant shoulder should be avoided, the implant was placed one millimeter lower than planned in this case (Fig. 3). After insertion of the healing cap (Fig. 3 below), the wound margins were adapted for transmucosal healing (Fig. 4). After ten days the sutures were removed.
Usually, ceramic implants are also reopened after a healing phase of three months. In this case, a four-month wait was required for safety reasons because the alveolar socket was not yet completely ossified. But even here the radiographic control image (Fig. 5, see first x-ray from left) did not show complete radiological healing of the alveolar socket, but the implant was osseointegrated and stable (Fig. 6).

Fig. 7: Precise impression taking through open impression.

Fig. 8: Customized abutment.

Fig. 9: Monolythic zirconium crown with occlusal screw connection on the master model (red screw = laboratory screw).

Fig. 10: Sealing the screw channel in the abutment with Teflon tape in preparation for bonding.

Fig. 11: Restoration bonded in situ, Teflon tape already removed by screw channel.

Fig. 12: Extraoral cement removal and polishing.
Prosthetic phase
The impression was taken in the usual way using a closed impression (Fig. 7). As it is a two-part system, the abutment can be adapted to the requirements and customized by grinding (Fig. 8). The external hex of the implant allows exact repositioning of the abutment, serves as a rotation lock and prevents forces from being introduced into the implant body. The connecting screw consists of a PEEK matrix with a 60 % proportion of embedded carbon fibers. This material allows a tightening torque of the screws of up to 85 Ncm, whereby 25 – 30 Ncm is clinically recommended. A monolytic zirconium crown (Fig. 9) (Zolid FX, Amman Girrbach) with occlusal access to the screw channel was fabricated on the customized abutment using the CAD/CAM technique (Studio für Zahntechnik, D. Tartsch).
To avoid possible internal tensions of the ceramic implant-abutment connection, the completed restoration was bonded to the abutment intraorally in the patient’s mouth in the same way as a titanium adhesive base [RelyX unicem, 3M ESPE] (Figs. 10, 11). The restoration bonded to the abutment can now be removed, excess cement safely removed and the transition polished (Fig. 12). For the final insertion, the tightening torque of 35 Ncm specified for the abutment screw must be observed. After filling the screw channel with Teflon tape, the access cavity is closed with composite as usual (Fig. 13).
The result is a metal- and cementless, screw-retained and reversible single-tooth restoration (Fig. 14). A radiographic control image was taken 4 months postoperatively before re-entry to check the gap-free and thus tension-free fit of the restoration after insertion (Fig. 5 left, centre). The radiographic control image as part of the follow-up after 2 years also shows stable peri-implant bone conditions (Fig. 5 right).

Fig. 13: Sealing the screw channel in the abutment with Teflon tape in preparation for bonding.

Fig. 14: Crown with composite closure of the screw channel
Conclusion
In addition to evidence and safe use, the possibility of being able to fall back on proven and familiar treatment protocols is an important factor for the acceptance of a new technology. On the basis of the described case it could be shown that these treatment procedures with two-piece ceramic implants hardly differ from the known treatment protocols with titanium implants. Indications and manufacturer’s guidelines must be taken into account accordingly.
Gallery
click to enlarge

No Comments