26 May PUBLICTwo-piece zirconium oxide implants with PEEK abutment

Two-piece zirconium oxide implants with PEEK abutment
Clinical situation
The patient came to the practice with functional problems due to nonocclusion in the posterior region and an overloaded front. The anterior bridge had already been heavily ground in alio loco. Two years later the bridge fractured. Clinical and radiographic diagnostics by means of OPG showed the deeper fractures of the root-filled abutment teeth 21 and 24. A bridge restoration over the curvature of the jaw arch is problematic in the absence of a canine tooth, especially with additionally increased lateral forces in case of a deep bite.
The patient decided on a restoration with ceramic implants.

The procedure

Fig 1: Initial situation: Due to the unfavorable abutment distribution and the patient’s deep bite, a leverage effect was created via the missing canine tooth 23.
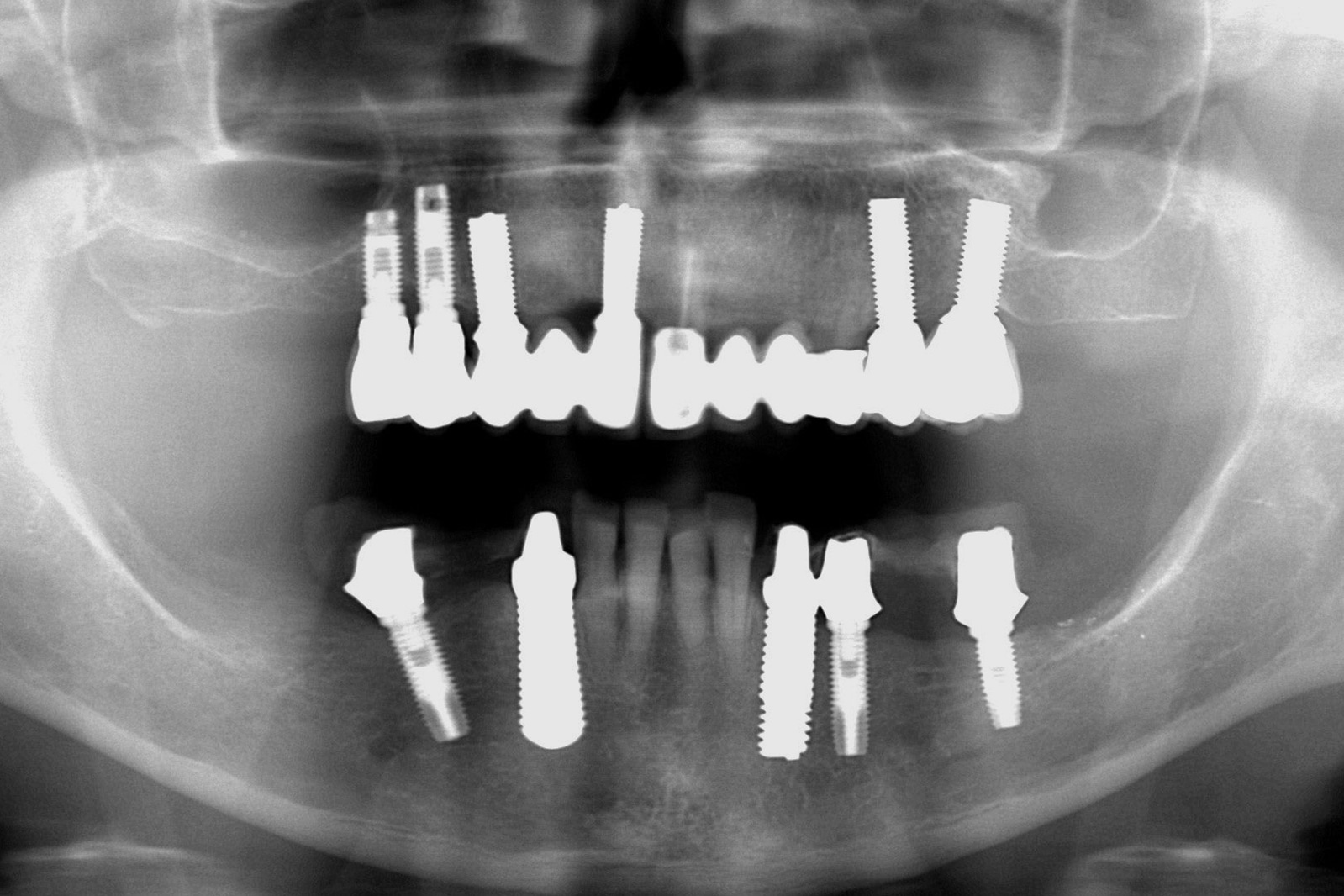
Fig 2: The abutment tooth 21 was root resected, both teeth 21 and 24 were fractured and root-filled.
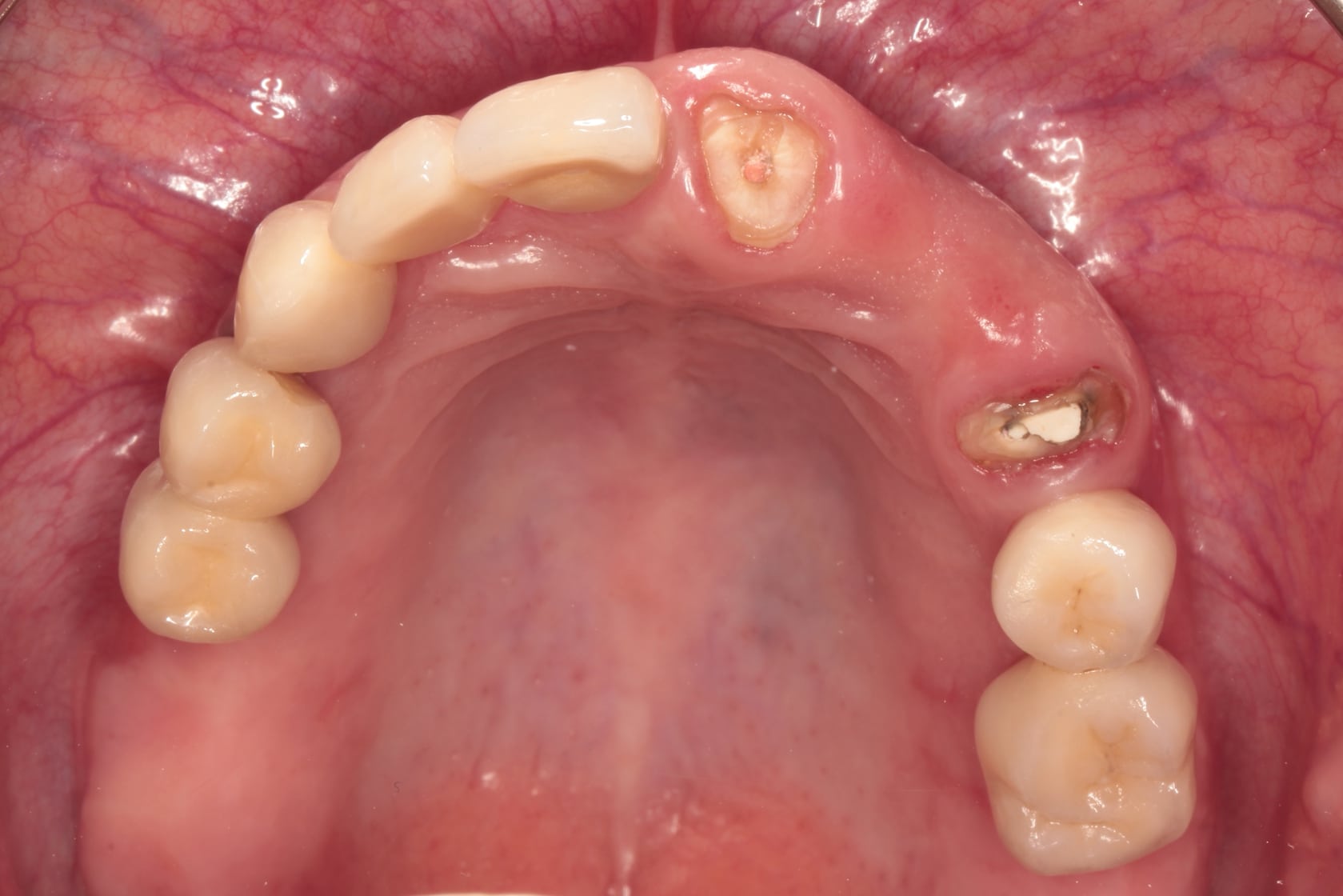
Fig 3: Condition after fracture of the bridge restoration due to the non-physiological load. Teeth 21 and 24 were not worth preserving, but were initially left in place to support bone and soft tissue.
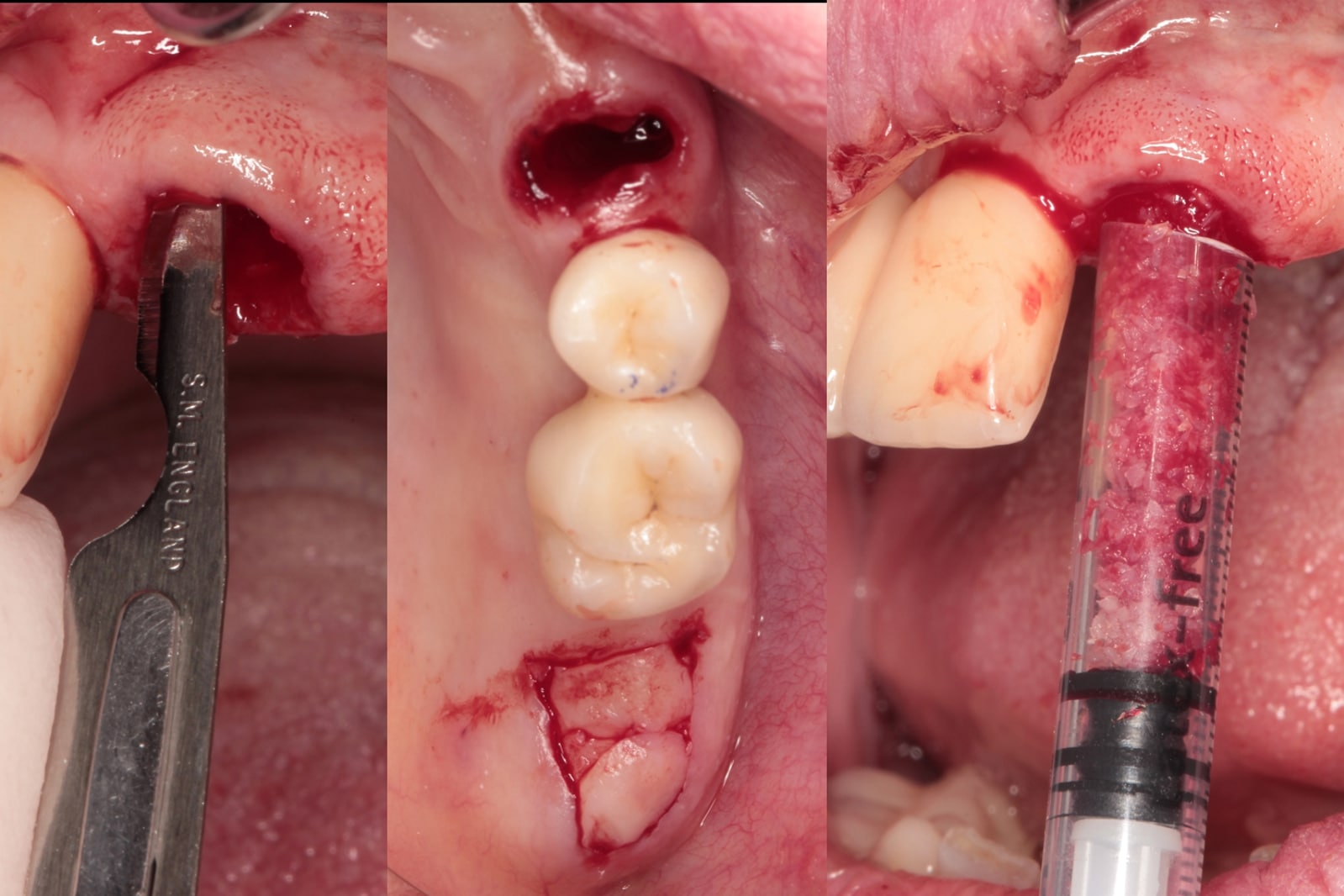
Fig 4: Augmentation and filling of the extraction sockets region 21 and 24 with a particulate allogeneic cancellous bone (DBM, osteograft) in the sense of ridge preservation.

Fig 5: The soft tissue graft was pulled into the previously labially prepared pocket by means of a tension suture. This ensured the nutrition of the graft and broadened the biotype.

Fig 6: Healing state after one month.

Fig 7: The garland-shaped incision helped to mark the implant positions during further treatment.
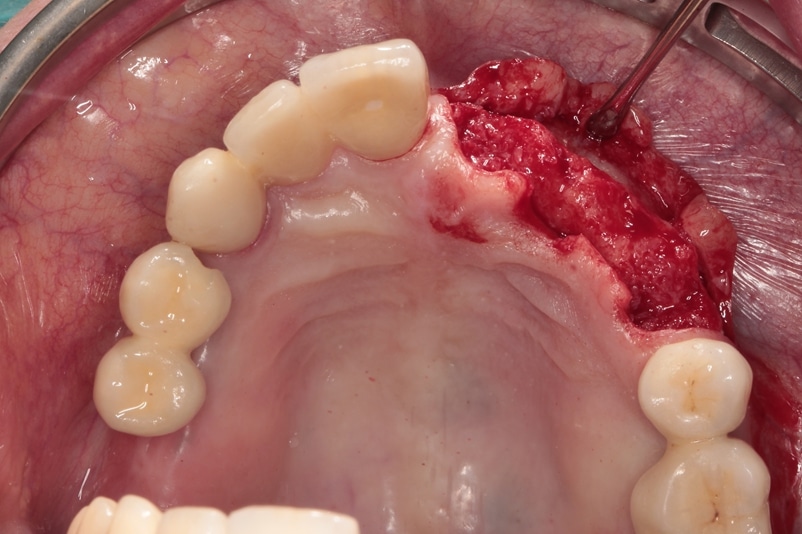
Fig 8: Exposure of the alveolar ridge and view of the well regenerated bone contour.

Fig 9: The prosthetic template served as an aid for locating the ideal implant insertion positions and for making the incisions.
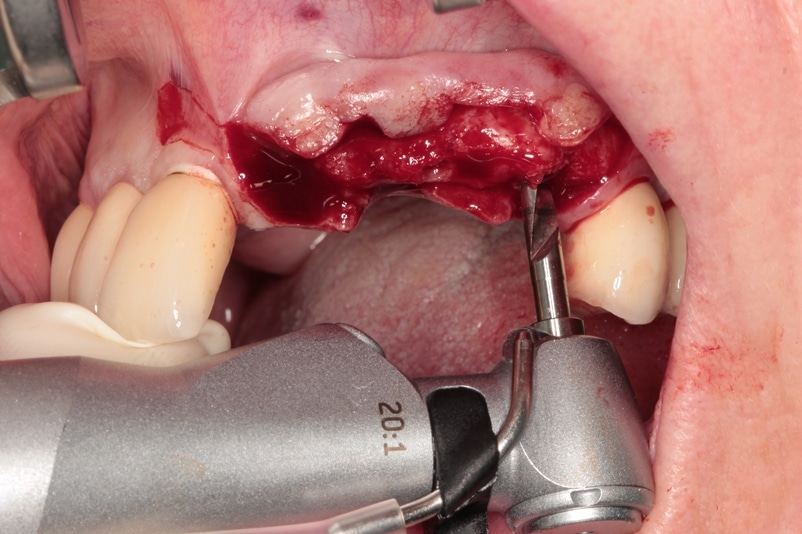
Fig 10: Step by step and with iChiropro (Bien Air) controlled speed were …

Fig 11: … the drilling operations are carried out safely and comprehensibly. The control was carried out by direction gauges.

Fig 12: The ceramic implants were inserted one after the other, starting in region 24, with the corresponding torques (26 Ncm, 33 Ncm, 24 Ncm).
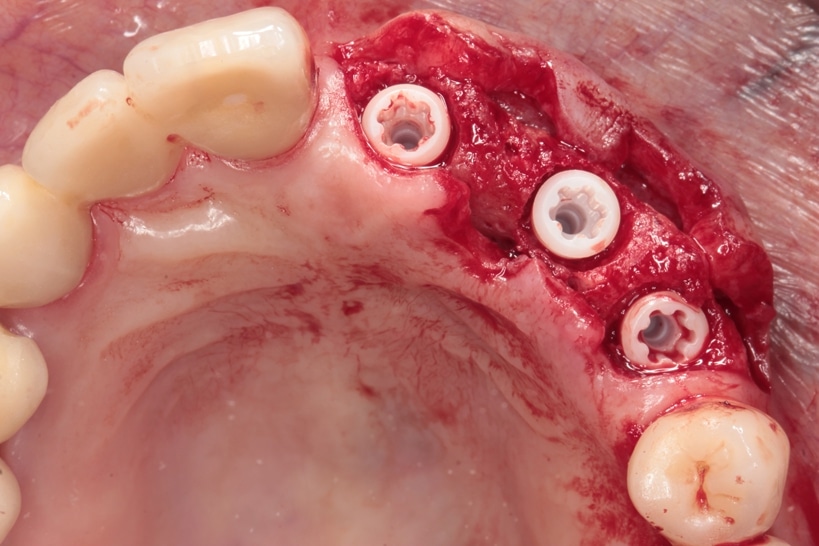
Fig 13: The implant shoulder is positioned 0.5 to 2mm supracrestally, depending on tissue thickness and abutment shape.

Fig 14: X-ray control post implantationem: The implant in region 24 was placed in connection with the anterior angled position of the implant 25.

Fig 15: Fixation of the soft tissue for closed healing with tension-free sutures.

Fig 16: Condition before exposure of the implants.

Fig 17: The exposure and simultaneous preparation of the rolling flaps was performed with a scalpel.

Fig 18: Condition six weeks after healing of the soft tissue.

Fig 19: The soft tissue around the Ceralog implants is stable after one year with the PEKK Abutments.

Fig 20: Impression of the impression posts with addition-cured silicone

Fig 21: The master model with PEEK abutments

Fig 22: Precisely fitting PEKK abutments, these should first be tested by the patient.

Fig 23: The brown discoloration on tooth 11 resulted from a gap between the bridge abutment and crown of an old restoration. This gap was repaired during the course of the treatment.

Fig 24: The X-ray control shows stable bone conditions after 1 year. The PEKK abutment is not radiopaque.

Fig 26: The definitive bridge restoration after 1 year
Conclusion
Zirconium oxide implants are considered a viable alternative to titanium implants.
As shown in the present case, better aesthetics and biocompatibility seem to be the main reasons for the alternative use of zirconium oxide
Case Gallery
Click to enlarge















No Comments